
Due to its widespread and free availability and research supporting its cost-effectiveness, Alcoholics Anonymous (AA) has been described as the closest thing public health has to a “free lunch”. Yet, not everyone may want a seat at the lunch table or want what’s on AA’s menu. This nationally representative study examined who is more or less likely to engage with AA.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Alcoholics Anonymous (AA) is a widely available recovery support option in the US and globally. Research using sophisticated research approaches show that in community-based AA, attendance – and especially more active involvement (e.g., working with a sponsor, socializing with other members, etc.) – promotes better alcohol and other drug use outcomes. Randomized controlled trials testing interventions that facilitate AA attendance – called 12-step facilitation – do as well as, or better than, other psychosocial approaches like cognitive-behavioral therapy in addressing alcohol use disorder, by engaging patients with AA in the community as intended. However, some evidence suggests that groups of people with alcohol use disorder may be more likely to participate than others. For example, among those with alcohol use disorder, minority women (compared to white women and men overall) and emerging adults (compared to “established” adults 30+) may be less likely to attend AA, beyond their lower rates of treatment-seeking more generally, but appear to benefit as much as older adults when they do attend. At the same time, treatment studies have shown Black patients are as likely as White patients to attend AA, while others show women are as likely as men to attend AA and benefit as much as men.
Examining whether certain subgroups are more or less likely to attend AA is critical because they are cost-effective recovery support options. If disparities are identified, future work can help uncover reasons for lower rates of AA attendance to inform future mutual-help facilitation incorporating the plethora of community options. The current study used nationally representative survey data from 2000–2020 to investigate whether lifetime AA attendance among those with a lifetime alcohol use disorder was associated with gender, race/ethnicity, and age.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the National Alcohol Survey (NAS). This nationally representative survey is conducted approximately every 5 years to collect data on rates of alcohol use and related health outcomes among the adult US population. Current analyses pooled cross-sectional data from 5 waves (2000, 2005, 2010, 2015, 2020). The analyses compared any AA attendance among participants with a lifetime alcohol use disorder. Participants included in the analyses (N=8,876) were: 1) 18+ years of age; 2) identified as non-Hispanic White, non-Hispanic Black, or Hispanic/Latinx; 3) completed all survey measures, who 4) endorsed 2+ symptoms of lifetime alcohol use disorder according to the DSM-5. The research team used a process to account for slightly different substance use disorder criteria between the DSM-IV used in 2000, 2005, and 2010 surveys removing the legal consequences criteria and employing other measures to determine the presence of alcohol craving.
Surveys assessed ethnicity via the question, “Are you Hispanic, Latino/a, or of
Spanish origin?” (yes or no). Race was assessed separately via the question “What is your race?” followed by response options including Black (or African American), White, American Indian, or Alaska Native, and other. Responses were combined to create a single variable indicating identification as non-Hispanic White, Latinx/Hispanic (any race), non-Hispanic Black/ African American. Surveys also asked participants’ age, which was categorized into emerging adult (ages 18–29) established adult (ages 30–64) or older adult (65+) categories.
The analyses also accounted for alcohol use disorder severity, professional treatment, and survey year. Substance use disorder treatment was measured via different survey questions depending on survey version. For surveys conducted from 2000–2015, lifetime treatment was assessed with the question: “Have you ever received treatment from a substance abuse treatment program (‘chemical dependency or substance abuse treatment program’ in earlier surveys) for either alcohol or drugs?” (yes or no). For surveys conducted in 2020, lifetime substance use disorder treatment was coded positive based on an affirmative response to this first question and/or an affirmative response to other similar items.
For determining lifetime AA attendance, participants were asked if “Have you ever gone to anyone—a physician, AA, a treatment agency, anyone at all—for a problem related in any way to your drinking?”. Those who endorsed yes to this question were either presented with a list of services they could have utilized (including AA) and asked to select all services they had ever used or asked explicitly “Did you go to a mutual-help group, such as Alcoholics Anonymous?” depending on the survey year. Responses to these measures were then categorized into yes (ever attended an AA meeting) or no (never attended an AA meeting).
Most of the sample self-identified as non-Hispanic White (77%) followed by Latinx/Hispanic (13.2%) and Black/African American (9.8%). Almost two-thirds of participants identified as male (60.8%). Participants were in 1 of 3 age categories: 18-29 years of age (24.7%), 30-64 years of age (67.5%) or 64+ years of age (7.9%). Most participants were married or cohabitating (61.6%), had completed at least some college (63.1%), and were employed (69%) at the time of survey administration. Most participants had never sought substance use disorder treatment (88.7%).
WHAT DID THIS STUDY FIND?
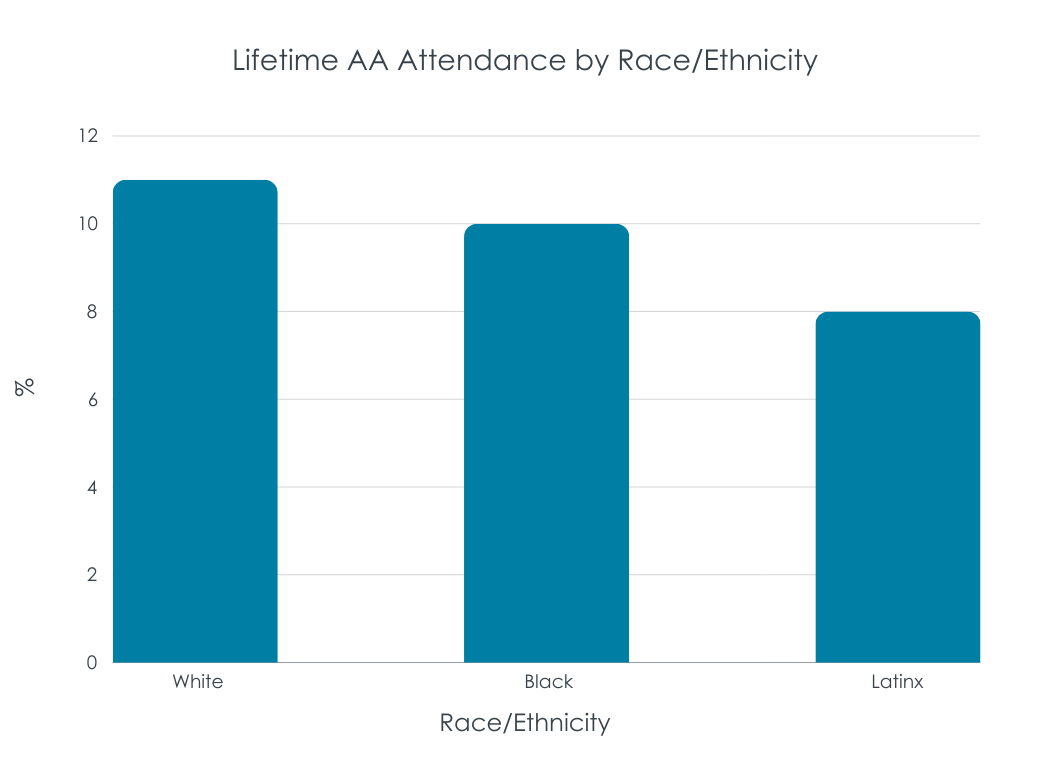
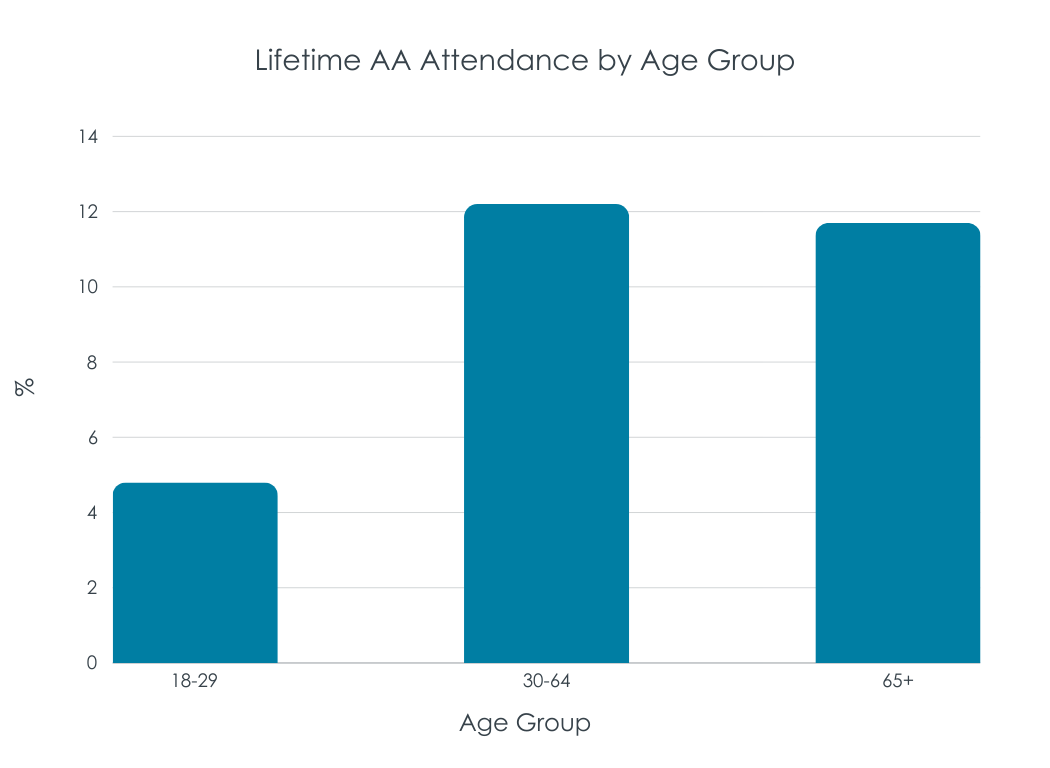
Race/ethnicity and age, but not gender, associated with AA attendance
Participants who identified as Non-Hispanic Black/African American were 41% less likely to have attended Alcoholics Anonymous meetings during their life relative to self-identified White participants. Hispanic/Latinx participants were 37% less likely to have attended Alcoholics Anonymous meetings during their life relative to White. These differences persisted when adjusting for alcohol use severity and utilization of addiction treatments. Those ages 18-29 were 65% less likely to attend AA than adults ages 30-64. These differences persisted when adjusting for alcohol use severity and utilization of addiction treatments. For gender, female identity was associated with lower AA attendance overall, but not after adjusting for severity and utilization of addiction treatment.
AA attendance group differences were consistent over time
These observed differences (or lack thereof in the case of gender) in AA attendance was present over time. That is, racial/ethnic minority and emerging adult participants were less likely to attend AA for each of the 5 surveys from 2000 to 2020.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that one’s propensity to attend AA in the US may differ by racial/ethnic and age groups, but not by gender. These findings are consistent with other nationally representative studies suggesting that Black individuals with substance use disorder may not attend AA and other 12-step mutual-help groups as often as White people. On the other hand, in a nationally representative sample of individuals who resolved a substance use problem, Black individuals were equally likely to have weekly or greater attendance at 12-step mutual-help groups. Another study with this sample showed that, compared to White participants, Black participants were more likely to use religious and spiritual practices and to view them as “making all the difference” in helping to resolve their substance use problem. Also, studies of individuals with a history of alcohol use disorder that examine AA alongside other mutual-help groups suggest Black and other minority individuals may be less likely than White individuals to attend “second-wave” groups, which include newer, primarily secular, mutual-help options like SMART Recovery. Given the high stakes of potential disparities in attendance at free, community-based mutual-help groups, research is needed to more fully understand the perspectives of racial/ethnic minorities, including but not limited to Black and Latinx individuals, and to examine different forms and degrees of mutual-help participation, including attendance and active involvement over time.
Young (e.g., “emerging”) adult status is a more consistent marker of reduced engagement with AA than any race/ethnicity identifications. While study analyses accounted for alcohol use disorder severity – lower, on average, in emerging adults – it may be more challenging for this age group to engage with groups that have many older members. Indeed, when emerging adults attend more meetings with young people, they have initially higher levels of attendance. That said, among those who do go, they benefit as much as their older (30+) counterparts. Clinicians may engage their emerging adult patients more readily with AA, and thereby improve outcomes, by helping link them with young adult specific meetings. Other innovative strategies too for this age group, including online recovery supports, are important to examine.
By learning scientifically about the specific mutual-help preferences and outcomes of key groups that have traditionally faced even more challenges than their White, older counterparts, public health and clinical guidelines can be better tailored to engage as many individuals with alcohol and other drug use disorder as possible with these freely available community-based supports or help identify other suitable options.



