Young people with attention deficit hyperactivity disorder (ADHD) have increased risk of earlier, risky substance use and for later developing substance use disorder compared to their peers without ADHD. Yet, timely ADHD treatment can help reduce risk for later substance use problems. This study examined whether a school-based ADHD intervention for adolescents improved alcohol and other drug use outcomes as these individuals entered young adulthood.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Nearly 1 in 10 youth globally and in the US meet criteria for ADHD. — ADHD is a neurodevelopmental disorder that has high variation across individuals but is often characterized by persistent, age-inappropriate, and disruptive levels of inattention, hyperactivity, and impulsivity. Specific difficulties may include negative outcomes in academic, social, neuropsychological, and affective domains, and individuals with ADHD are at an elevated risk of starting substance use earlier and later developing a substance use disorder compared to their peers without ADHD. The connection between ADHD and substance use disorders is explained by several potential contributors including shared dopamine system dysregulation, high impulsivity, peer influences, and self-medication of symptoms.
There are many skills-based, pharmacological, and behavioral treatments shown to improve ADHD symptoms; however, few have assessed substance use outcomes. Emerging evidence suggests that psychosocial treatments have the potential to address both ADHD and substance use, while robust research demonstrates their effectiveness in improving individual, familial, and academic outcomes. This highlights the possibility that ADHD-focused interventions could also lead to improved substance use outcomes for youth with ADHD.
The researchers in the current study designed a school-based training intervention for adolescents with ADHD to improve academics and the social difficulties of adolescence, including problem-solving, organization, study, social, and planning skills. The program was shown to improve factors such as academic performance and social skills in a previous evaluation of the intervention. Given the well documented added risk for substance use among those with ADHD, treating ADHD may also reduce substance use both concurrently and over time. The present study investigated if this school-based ADHD intervention improved substance use disorder symptoms among adolescents with ADHD both immediately following the intervention, 6 months later, and at 5-year follow-up when these participants reached young adulthood.
HOW WAS THIS STUDY CONDUCTED?
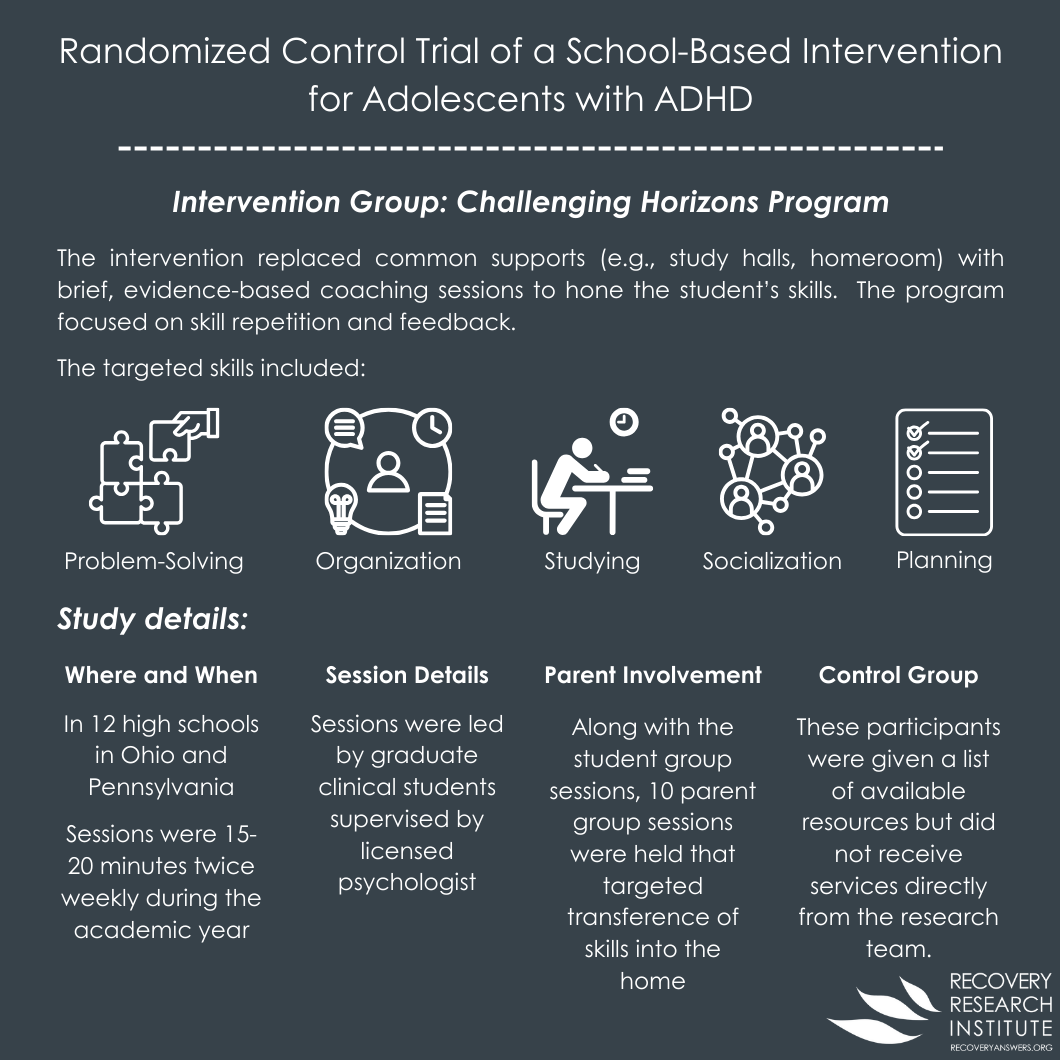
This study was a secondary analysis of data from a randomized control trial of a school-based intervention versus a community care comparison receiving only a resource list for adolescents in grades 9-11 with ADHD. The intervention, called Challenging Horizons Program, targeted skills including problem-solving, organization, study skills, problem solving, and social functioning. See figure below for a detailed description.
In brief, the intervention was embedded within 12 high schools in Ohio and Pennsylvania replacing common academic supports (e.g., study halls, homeroom) with brief, evidence-based coaching sessions to hone the student’s skills. The sessions were led by graduate clinical students supervised by licensed psychologist and lasted between 15-20 minutes twice weekly throughout the academic year. About 80% of students attended at least 30 sessions. There were also 10 group sessions held in the evenings throughout the year. Concurrent to the student group sessions, 10 parent group sessions were held that targeted transference of skills into the home (both academic and socio-relational). The intervention was found to improve several domains related to ADHD, such as academics, organization skills, and social skills.
The original sample included 185 adolescents that met criteria for ADHD, had an IQ of 75 or above, did not have bipolar, psychotic, or obsessive-compulsive disorders, and did not exhibit alcohol or other drug use disorder symptoms. Students were evaluated prior to treatment, immediately after treatment (about 11 months after treatment initiation), 6 months following treatment completions (about 18 months after treatment initiation), and 5 years after treatment completion. The randomized control trial occurred 2015-2018, with the long-term follow-up occurring 2021-2022.
Problematic alcohol use was assessed with the Face-Valid Alcohol subscale from the adolescent self-report Substance Abuse Subtle Screening Inventory-A2 (SASSI-A2) at the baseline, post-treatment, and 6-month follow-up. Alcohol use was assessed with the Alcohol Use Disorders Identification Test (AUDIT) for the long term (5-year) follow up. For both measures, higher scores reflect more problematic alcohol use. Substance use was initially assessed with the Face Valid Other Drugs (FVOD) subscale of the SASSI-A2, and then it was measured with the Drug Use Disorders Identification Test (DUDIT) at the long-term follow-up. As authors state, the switch in measures for alcohol and substance use were made to ease participant burden, gather additional information, and reduce assessment costs. However, the change in measures does introduce a limitation in comparing the various timepoints as well as interpreting the trends in use.
Analyses were conducted to test the ADHD intervention’s effects separately on both the likelihood of any substance use and, among those with any use, the degree of substance use for a) alcohol and b) other drug use. Analyses controlled statistically for participant gender, age when beginning the study, time since they received study treatment, baseline level of the outcome variable (alcohol or drug use), parent alcohol/drug use, and the additional presence of oppositional defiant disorder. Because there was variation in outcomes at the school level, additional statistical controls were employed to adjust for those school-level differences. Also, only 144 were retained at post-treatment, 124 at 6-month follow-up, and 73 for the long-term follow-up. Analyses included 184 individuals for alcohol use analyses and 183-185 for drug use analyses (removing some they determined to be outliers). Authors used a statistical approach to estimate the trajectories of all individuals, even those individuals who did not complete follow-ups. Those at follow-up were more likely to be girls (29% vs 21%) and less likely to identify as Hispanic (5% vs 11%) – of note analyses did not control for race/ethnicity.
WHAT DID THIS STUDY FIND?
ADHD intervention did not improve alcohol use, associated with worse alcohol problems
There were no group differences on alcohol use (yes/no) over time – across the entire sample, 18% reported alcohol use at post-treatment, 23% at 6-month, and 76% at long-term follow up. Among those who drank alcohol at the long-term follow-up, the intervention group had a small but statistically significant disadvantage on alcohol use problems. Additional exploratory analyses were done to investigate these counterintuitive results. Those in the treatment group were found to be more likely to meet criteria for risky alcohol use, and each item on the alcohol use disorder identification test (AUDIT) was examined for differences between treatment group. Four out of the ten alcohol measure items were different between the groups. There was also a relationship between more social skills at the 6-month follow-up and more subsequent alcohol use among those in the treatment condition as well as more alcohol problems at the long-term follow-up compared to their peers.
ADHD intervention did not improve any drug use, but did reduce drug use problems at the 6-month follow-up
The intervention and comparison groups had similar rates of drug use other than alcohol over time – across the whole sample, 19%, 21%, and 35% reported drug use at post-treatment, 6-month, and 5-year follow-ups, respectively. That said, adolescents who reported any drug use at the 6-month follow-up had moderately fewer drug use related problems.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results from this secondary analysis of a school-based ADHD intervention among adolescents with ADHD found limited support of secondary effects on substance use outcomes. The intervention was not associated with alcohol or other drug use at post-treatment, 6-month follow-up, or the 5-year follow-up. The intervention was found to produce modestly lower drug use problem scores among those that reported any drug use at the 6-month follow-up, but not the other time points. Counterintuitively, the intervention was associated with more alcohol use problems among those with any alcohol use at the 5-year follow-up. Identifying prospectively how and for whom any improvements in ADHD symptoms are related to changes in alcohol and drug use may help tailor future interventions for adolescents with ADHD, who are at a heightened risk of substance use.
There were several positive outcomes of the ADHD intervention from the primary study findings, including improved social skills and academics. The researchers hypothesized that the intervention would similarly improve underlying mechanisms that contribute to substance use (e.g., self-esteem, problem solving, planning, social skills). However, this was not borne out in the findings.
Not only did the intervention produce similar alcohol and other drug use rates, but the intervention unexpectedly led to more alcohol use problems among those with any alcohol use 5-years after the intervention. One possible explanation presented by the research team from exploratory analyses was that higher social skills were linked with more alcohol-related problems. In a previous study, with the same participants, greater emotional skills were associated with greater social skills, which were then associated with a higher likelihood of problematic alcohol use. Thus, the improvement in social skills from the ADHD intervention may facilitate adolescents with ADHD to connect with peers who are more likely to drink (e.g., at social gatherings, etc.). The data and analyses do not suggest that the intervention causes more alcohol-related problems directly. Yet, the ADHD-related improvements from the intervention may counterintuitively pave the road for an alternate alcohol use pathway. Future study is needed to explore how and for whom the intervention facilitates this alternative alcohol use pathway as well as how to perhaps supplement the existing intervention with substance use specific modules to counteract these undesirable effects.
Finally, of note, some national data suggests people with ADHD who received treatment earlier and for a longer period have risk that is similar, or lower to their non-ADHD peers, though later medication onset or any non-medical use may increase risk – pointing to a more complicated relationship between ADHD stimulant medications and later substance use.
The results from this study should be considered in light of two very important key limitations:
• First, only 39% of the original participants completed the 5-year follow-up. Moreover, gender, ethnicity, and oppositional defiant disorder were all connected to who had missing data. The high level and non-random missingness may bias results. The researchers incorporated statistical techniques to minimize the bias, but such approaches do not eliminate the potential bias. Thus, the findings may not generalize to all adolescents with ADHD.
• Second, the researchers changed which alcohol and other substance use measures they used at the 5-year follow-up. Although the intentions were scientifically grounded, the findings may reflect differences between measures and not true differences in alcohol and substance use or related problems. Furthermore, the study was not designed to thoroughly investigate substance use. Additional steps may be needed in future intervention work to fully understand the role of ADHD and ADHD interventions on substance use.