
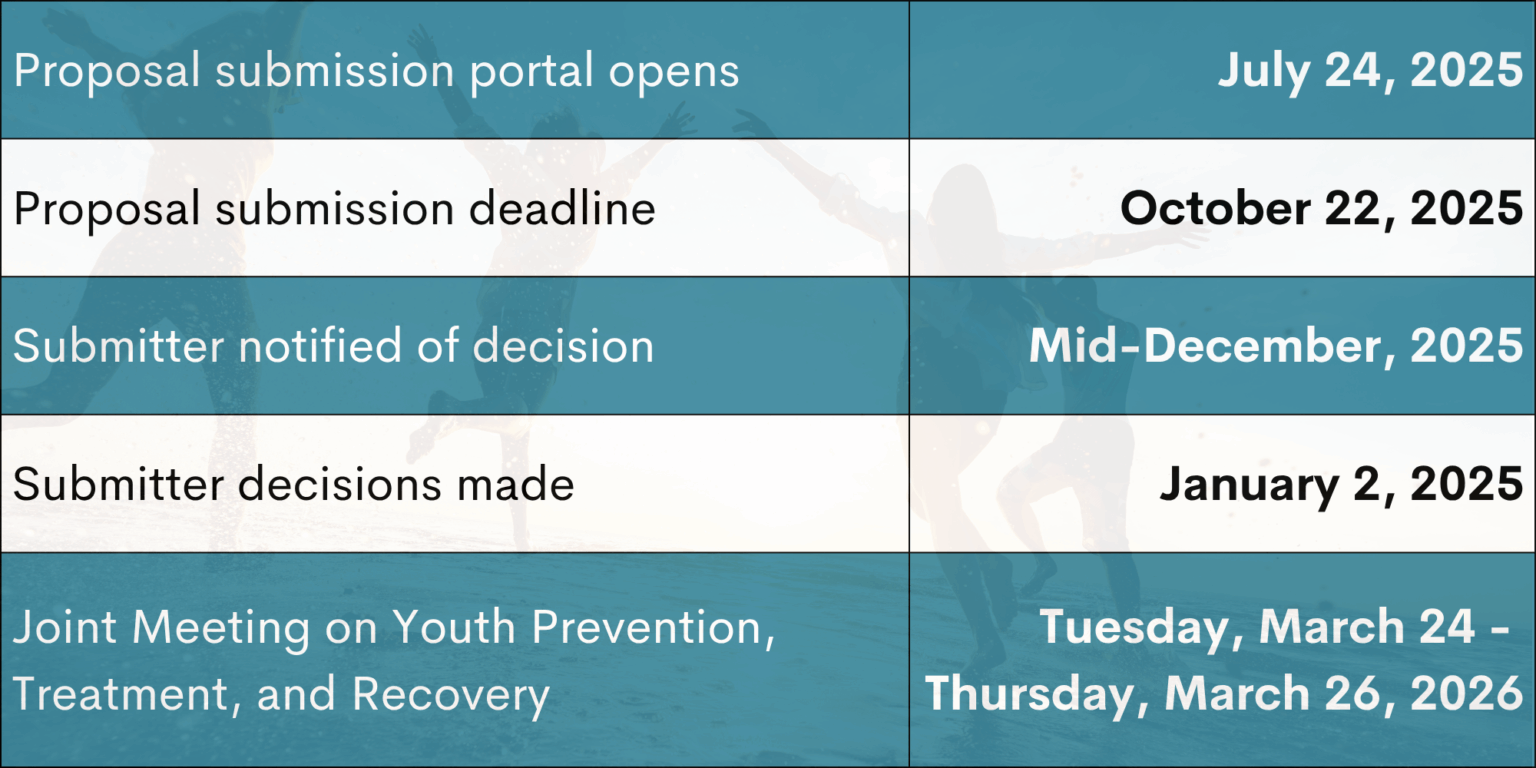
Thank you for submitting your proposal to the 2026 Joint Meeting on Youth Prevention, Treatment, and Recovery. The deadline to submit proposals has passed and the submission portal is closed.
The following information outlines the requirements and process for submitting a proposal to the 2026 Joint Meeting on Youth Prevention, Treatment, and Recovery (JMYPTR). We have updated this information from past years, please review all details carefully before preparing your submission, even if you have submitted to us before. Contact info@youthrecoveryanswers.org with any questions or concerns.
We strongly encourage proposals that elevate the voices of young people with lived experience. All inclusion of youth must be done ethically, with informed assent and parental consent (where appropriate) as well as appropriate support. Further, we trust that presenters will adequately ensure that youth participation is empowering, voluntary, and respectful of each young person’s boundaries and well-being.
Please note that those submitting presentations involving youth will be required to meet with the conference team in advance of the event to discuss your plan for youth engagement should the submission be accepted. This is done to provide additional guidance, support, and assistance for the presenter(s) when involving young people and/or their families.

The current alcohol and drug crisis in our nation is unprecedented – to address it, we need collaborative urgency, action, and innovation. There is an increased recognition of the need to prevent the onset of substance use disorders, intervene earlier in the clinical course, provide access to overdose prevention services, and engage young people much sooner with services that can help initiate, support, and maintain remission and stable recovery. The 2026 JMYPTR will serve as a platform for all stakeholders to gather, learn, and share information about evidence-based and innovative practices and research as well as foster new collaborations.
In this work, it is essential to recognize the disproportionate burden of substance use and its consequences among Native American youth. Structural inequities, historical trauma, and under-resourced systems have contributed to significant disparities in access to prevention, treatment, and recovery services for this population. JMYPTR is committed to centering the voices, experiences, and leadership of Native American youth and their communities to ensure that the solutions we develop are not only inclusive, but equitable and culturally grounded.
The current era of change spans many fields and cuts across multiple levels:
The 2026 JMYPTR features three distinct but overlapping tracks
Presentations are organized according to these general tracks, although presentations can span across more than one where necessary. When more than one track applies to a submission, authors should choose whichever one is most applicable. JMYPTR proposals should focus on children, adolescent, and emerging adult populations. See definitions on final page for more information.
This track seeks presentations focused on prevention and early interventions that aim to prevent and reduce overall harm immediately during the young person’s adolescent and emerging adult years as well as preventing lifelong problems. Suitable topics could include but are not limited to:

There is a pressing need to identify novel treatments and practices that have been developed specifically for youth, and for these to have been developed with youth and family input. This track seeks proposals of novel treatments and practices for which there may be theoretical support, pilot data, or early trial evidence of a positive effect on young people. Studies of existing treatments which seek to limit disparities among minority populations by adapting approaches to specific populations will be appropriate for this track. Proposals addressing the unique treatment needs of Native American youth and incorporating traditional or community-rooted healing practices are especially encouraged. Small sample studies or qualitative studies that have a strong theoretical rationale will also be appropriate for this concentration. Other topics to be addressed within this track could include such elements as:

The field has moved to valuing recovery-oriented systems of care, that is, a transformational shift in how we approach youth substance use prevention, treatment, and recovery. From this perspective, there should be “no wrong door to treatment” and no single pathway to recovery. A comprehensive infrastructure supporting both treatment and recovery must be developed. This concentration will focus on how the different and multiple youth- and family-serving systems can support youth through (1) evidence-based interventions, treatments, and practices, (2) education-based prevention and recovery supports, and (3) community-based recovery supports.
This track will also focus on different aspects of the larger continuum of care as well as proposals that examine infrastructure elements such as collaboration, integration, and supportive organization and financing arrangements across multiple systems that serve youth and their families. Proposals that highlight culturally grounded recovery pathways and community-led recovery supports for populations at elevated risk, including Native American youth, are especially welcome. Topics to be addressed within this concentration could focus on areas such as:
Recognizing that not all youth substance use submission topics fit neatly into one of these tracks, other presentation topics welcomed at the conference are included below. When deciding which track to submit, please classify your proposal as you see fit. Some of these topics include, but are not limited to, the following:
Below is a description of the session types and presentation categories featured in JMYPTR. Each submission should fall under one session type, and we are looking for presentations that fall under at least one of the following categories. All presentation types have a presenter count limit (i.e., only a maximum of X presenters are allowed to present at the conference itself), but are welcome to have as many co-authors as needed.
All submissions will be reviewed by at least 2 peer reviewers before a final decision is made. Submissions will be reviewed based on the following criteria:

Note: The conference adheres to the International Society of Addiction Journal Editors consensus statement which recommends against the use of terminology that can stigmatize people who use alcohol, drugs, other addictive substances or who have an addictive behavior (isaje.net/addiction-terminology.html). Please also see the Addictionary at recoveryanswers.org for guidance when developing proposals and final presentations.