
Contingency management is a helpful intervention for treatment-seeking adults with cannabis use problems in which participants receive immediate incentives (e.g., money) for demonstration of a given behavior (e.g., abstinence). This study investigated if a short-term cannabis contingency management intervention for young people not currently seeking treatment led to reduced cannabis use in the weeks after the intervention ended.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Among adolescents, cannabis is the second most used substance, only behind alcohol with 18% of adolescents in 2023 reporting cannabis use in the last year. Similarly, 37% of young adults aged 18-25 reported cannabis use in the past year. Cannabis use among young people can have short and long-term adverse effects. Compared to individuals with minimal cannabis exposure, individuals with heavy, frequent, or problematic cannabis use have been noted to have worse learning, attention, and executive functioning. It is also associated in young people with worse performance on tasks related to working memory, attention, and psychomotor speed. Adolescents with cannabis use disorder are also at an increased risk for suicide attempt or engaging in self-harm. The potential for adverse effects directly linked to cannabis is especially important because of the changing trends, potency, and availability of cannabis. Furthermore, the changing legal landscape (e.g., the legalization of recreational cannabis use) has led to decreased perceptions of cannabis use related harm among adolescents in many states.
Those engaging in cannabis use may seek or benefit from evidence-based treatments such as contingency management. Contingency management is a behavioral health intervention that can easily be integrated into existing treatment programs and delivered by behavioral health professionals. In contingency management interventions, rewards such as money are awarded rapidly to those that demonstrate objective evidence of a desired behavior (e.g., cannabis abstinence). Contingency management has among this strongest evidence for adults with substance use disorders. However, contingency management has had mixed results in treating cannabis use among adolescents and young adults.
Two critiques of contingency management are that 1) the positive effect of the intervention will end once there are no more rewards for the behavior and 2) only those actively seeking treatment will benefit. This study helped partially test these concerns by recruiting adolescents currently using cannabis but not seeking treatment as well as assessing any lasting effects of contingency management. The study specifically explored if successfully completing a cannabis abstinence contingency management intervention still showed benefits four weeks after the intervention ended among non-treatment seeking young people. The findings have implications for the use of contingency management among young people as both an intervention and harm reduction tool.
HOW WAS THIS STUDY CONDUCTED?
This study combined data from studies that recruited adolescents (13-18 years) and young adults (18-25 year) in the greater Boston area that used cannabis at least weekly, were not actively seeking treatment for cannabis use, had no immediate plans to reduce or discontinue their use, and were medically healthy, both of which randomized participants to rewards contingent on abstinence (i.e., contingency management group) or non-contingent rewards (i.e., monitoring group). The study period was 4 weeks of intervention or monitoring, at which point rewards for the contingency management group were removed and participants completed a follow-up assessment 2 to 4 weeks later. The initial clinical trials sought to explore the impact of cannabis abstinence on cognitive functioning among young cannabis users not seeking treatment.
Participants were randomized into a contingency management intervention or a control group that was only monitored. Participants randomized to the contingency management group were asked to immediately discontinue cannabis use, while those in the monitoring group were not asked to change their cannabis use. Individuals in the contingency management group that used cannabis in the first week were reminded of the abstinence requirement and given one more chance to remain in the study. Those that used cannabis again were removed from the study. This is noteworthy as it creates a group receiving contingency management that is systematically more drawn to abstinence; introducing a possible bias favoring intervention effects – i.e., sustaining abstinence even once the contingency management is removed.
Randomization was stratified by sex (male vs female), age, and average frequency of cannabis use to help achieve a balanced allocation of the participations, which reduces confounding variables and improves the comparability of the two groups. Cannabis use was assessed via self-report and biochemical verification. Participants were asked to report both the number of days and the number of times they used cannabis in the past 90 days (only at baseline) or since the last study visit. Biochemical verification was also obtained through a urinalysis to quantify THC concentration. Participants in the contingency management group were also asked about their cannabis use intentions at the end of the contingency management protocol: 1) remain completely abstinent from cannabis, 2) resume using, but less than I did before I started the study, 3) resume using at the same level as I did before I started the study, or 4) I want to resume using, but more than I did before I started the study. These four categories were then collapsed into “resume using at the same level or more” and “use less or abstain from cannabis use.”
The contingency management protocol consisted of increasing compensation for continued abstinence as well as attendance. The value of incentives escalated incrementally to encourage study retention and continued abstinence. Participants could receive a max payment of $545 or $420, depending on which clinical trial they were involved in (young adult vs adolescent). In the control group, participants were only compensated for study attendance. In either group, if a participant missed a visit, their payment would revert to the initial attendance payment level ($5).
A total of 102 (82%) young people in the contingency management group had biochemically verified continuous cannabis abstinence at the end of the 4-week intervention. The 23 participants in that intervention group who withdrew consent, resumed cannabis use, or dropped out of the intervention were younger, had higher cannabis use severity, used cannabis more frequently, and had higher THC concentrations compared to those that completed the intervention with continued cannabis abstinence. There were also 8 individuals in the contingency management group that did not complete the follow-up visit. There were 13 participants in the control group that did not complete the follow-up visit. There were 95 young people in the final contingency management group and 81 in the control group. The average age for the intervention and control groups were 20 and 19 years old, which was a statistically significant group difference. Both groups had 44-46% female individuals, and most (71% and 56%) identified as White. While a much larger percentage of contingency management participants were White, this group difference was not statistically significant. The average age of first cannabis use in both groups was 15. There were also 47 (50%) and 56 (68%) of participants with a cannabis use disorder in the intervention and control groups, respectively.
WHAT DID THIS STUDY FIND?
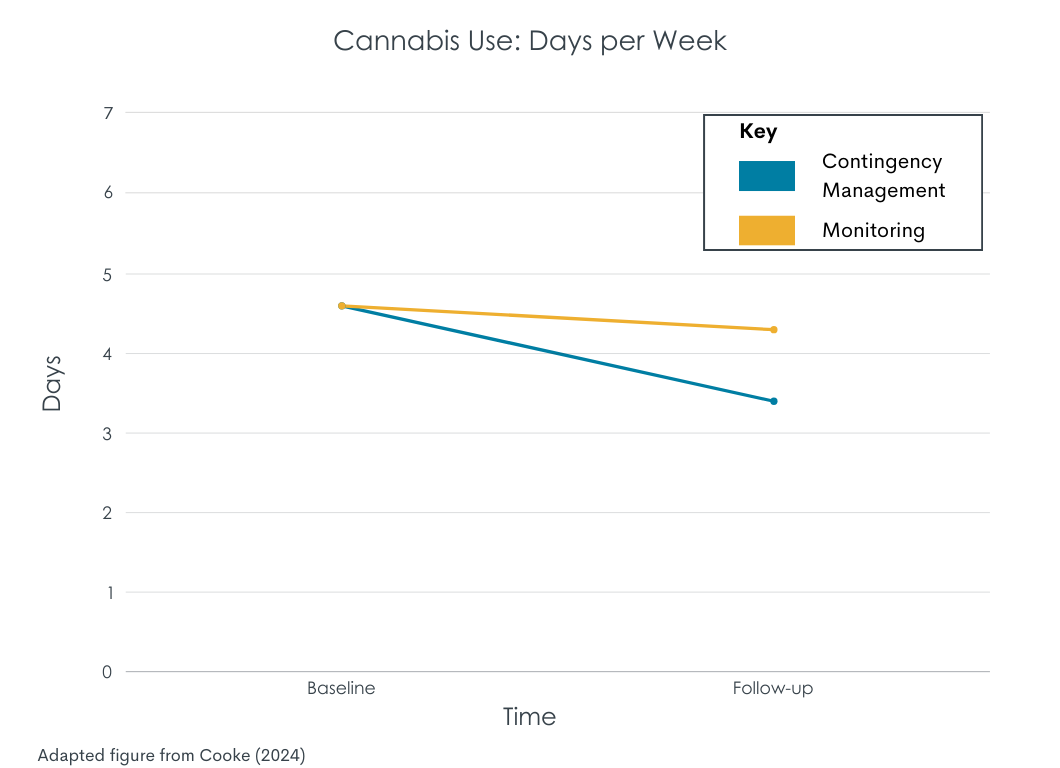
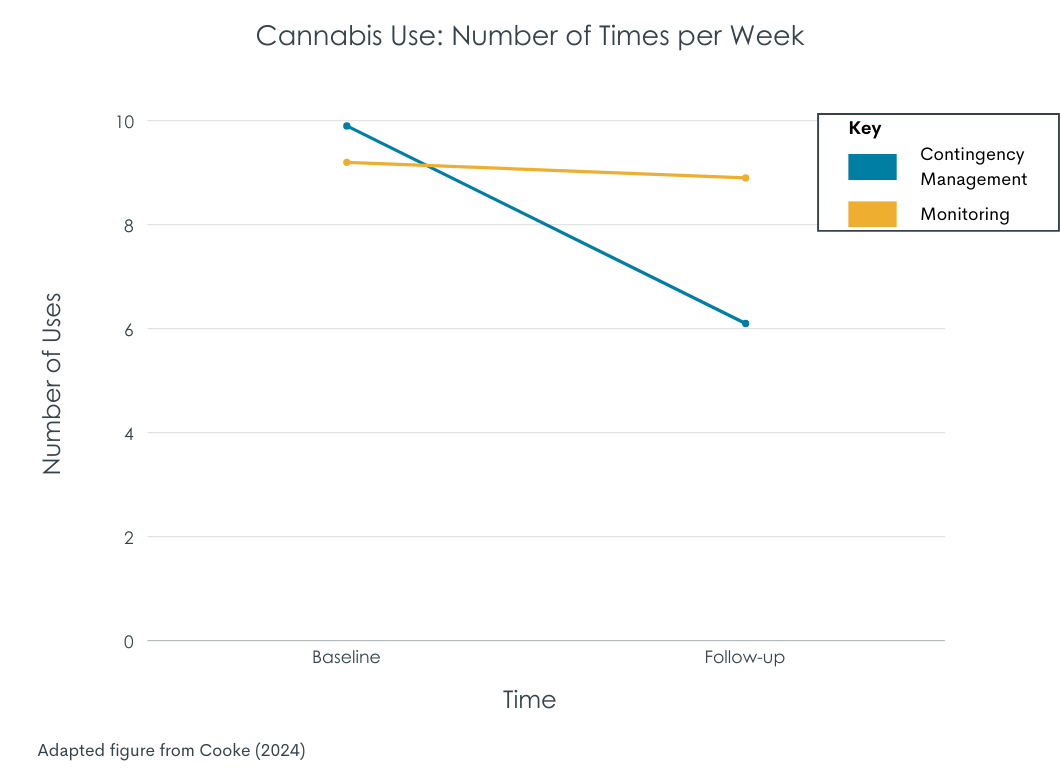
Contingency management completers had greater reductions in cannabis use that lasted through follow-up
Participants that completed the contingency management protocol—maintained 4 weeks of cannabis abstinence—reduced cannabis use after rewards were discontinued with 1.2 days less and 3.7 times less per week. The control group, however, did not reduce their use between baseline and follow-up. Approximately half of the contingency management group reported a decrease in days (50%) and times (55%) of weekly use by at least 20% from their baseline cannabis use. In addition to the self-reported reduction in use, contingency management completers had reduced THC concentrations from baseline to the follow-up.
Most contingency management completers wanted to use less cannabis after the intervention
Contingency management completers, but not control group participants, were asked at what level they’d like to use cannabis at the end of the contingency management intervention. The majority (68%) reported that they’d like to maintain cannabis abstinence or reduce their use compared to baseline levels. Those that identified a reduction goal wanted to reduce their use by an average of 2 days per week and 6 times per week compared to their baseline frequency of use. Setting a reduction goal was also associated with a reduction in days of cannabis use and THC concentrations at the follow-up. Those that set a reduction goal used, on average, about 2 days less compared to baseline.
Individuals without a cannabis use disorder had greater reductions
Among contingency management completers, 47 had a cannabis use disorder diagnosis and 44 did not. Individuals without cannabis use disorder reported on average 5 fewer times of cannabis use per week from baseline to follow-up, while those with a cannabis use disorder reported on average 3 fewer times of cannabis use per week. In contrast, those with a cannabis use disorder had greater reductions in THC concentrations from baseline to follow-up compared to those without a cannabis use disorder.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Contingency management interventions have been seen to increase abstinence among youth with substance use problems. Most intervention studies are short-term (a few months or less) and do not track substance use outcomes after the intervention period. Some critics suggest that the positive effects of contingency management will disappear once the incentives stop. The researchers in this study found that individuals who completed the contingency management intervention continued to have less frequent cannabis use and reduced THC concentrations, which is a biochemical marker of cannabis use at least through 2-4 weeks after the incentives were withdrawn. This suggests that contingency management, particularly for young people, may help reduce cannabis use even after the intervention ends at least in the short term. That said, an important confound here is that if participants assigned to receive contingency management were not able to abstain, they were removed from the study, creating a selection bias. As such, the contingency management group is referred to in the study as the “abstinence” condition; the sustained benefits may be related to the group’s enhanced propensity toward abstinence (by dropping those unable to achieve abstinence early on). Indeed, those who did not complete contingency management were younger and had more severe cannabis use.
That said, individuals incentivized to abstain, and were able to maintain abstinence for 4 weeks, had clear advantages on cannabis use 2 to 4 weeks later compared to a group receiving non-contingent rewards that were not required to abstain during the intervention. These youth who abstained from cannabis had “no immediate plans to reduce or discontinue cannabis use” when entering the study. This suggests some benefit of contingency management facilitated abstinence that extends beyond the rewards themselves. It is possible that abstinence (facilitated by rewards) gave participants the opportunity to experience abstinence for a while and this could have independently and indirectly enhanced their abstinence motivation, self-efficacy, and coping skills – mechanisms explaining benefit from other treatment and recovery supports – despite the treatment not targeting these processes directly. Though mechanisms explaining cannabis reductions were not tested in this study.
The researchers also found that participants without a cannabis use disorder had greater reductions in times per week of cannabis use compared to those without a cannabis use disorder. These findings regarding cannabis use in non-treatment seeking youth contrast with a systematic review of contingency management for adults with opioid or stimulant use disorders, which showed contingency management to be more beneficial for those with more severe and/or complex clinical presentations. More work is needed to understand the how and for whom cannabis contingency management has positive effects.



