Adolescence is a pivotal developmental growth period. Although the World Mental Health assessment called the “Composite International Diagnostic Interview Substance Abuse Module” (CIDI-SAM) was developed for adults, it is commonly used with adolescents. Thus, it may not accurately or reliably identify adolescents with substance use disorders. This study compared this module to diagnoses made by experienced clinicians.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Alcohol and other drug use among adolescents can be particularly harmful given adolescence is such a critical developmental period in the human life course. Substance use can disrupt healthy biological, emotional, and social development. Many adolescents engage in some form of substance use, and, for some, substance use is associated with life-altering consequences, such as delayed workforce entry, academic problems, later substance use and other psychiatric disorders, and injury or death.
Clinicians need reliable and valid assessment tools to identify adolescents with a substance use disorder and then to deliver appropriate treatments. Public health and policy experts also rely on valid measures of substance use disorders to understand trends of substance use disorder and develop relevant policies.
The World Health Organization developed a comprehensive survey tool to obtain valid information across 28 countries about the prevalence and correlates of mental health disorders, unmet need for treatment, treatment adequacy, and the societal burden of mental disorders. The survey included a substance use disorder module to specifically evaluate substance use. The substance use module is often used as the standard in research and practice to diagnosis substance use disorders. However, the module has not been validated with adolescents. How well the assessment compares to trained clinical experts in diagnosing substance use disorder among adolescents is unknown. Thus, researchers in this study aimed to compare diagnoses between this substance use module and clinical experts. Studies like these can also help us understand how accurate clinicians are in their real-world diagnostic assessments of substance use disorder for youth.
HOW WAS THIS STUDY CONDUCTED?
This cross-sectional study recruited adolescents from one outpatient substance use disorder clinic between July 2020 and February 2022. All adolescents aged 12-17 years were invited to participate in a study exploring the properties of substance use screening tools for adolescents. Among the 280 eligible participants, 38 adolescents chose to participate and completed the study. About two-thirds of participants (26, 68%) identified as male, and the average age was 16. About three-quarters (29, 76%) identified as White, and 32 (84%) identified as non-Hispanic. Participating adolescents were primarily from a home with two or more caregivers (31, 82%), with 27 (71%) homes having a caregiver with a college education or higher. Many (17, 45%) adolescents self-reported a history of being diagnosed with, or receiving medication for, attention deficit disorder/addition deficit hyperactivity disorder, and one-quarter screened positive for depression based on the PHQ-2 (10, 26%), and one-quarter also screened positive for generalized anxiety disorder based on the GAD-2 (9, 24%).
The 38 adolescents were given the web-based, World Mental Health Composite International Diagnostic Interview Substance Abuse Module (referred to in this summary simply as “module”) by a trained research assistant. They then underwent a 60-minute pediatric addiction medicine telehealth evaluation. The evaluating clinician was not made aware of the module results.
The evaluation was guided by a template that included open-ended prompts asking why the adolescent was seeking evaluation, what they hoped to gain, and what they liked/disliked about substance use. The guide also included a list of the substance use disorder criteria from the Diagnostic and Statistical Manual of Mental Disorders, 5th edition. The 11 criteria for substance use disorders were assessed separately for alcohol, cannabis, and tobacco use disorders. Results from the module and clinician evaluations were then compared. In this study, a clinician’s diagnosis was assumed to be accurate and the “gold standard”. The module’s ability to correctly identify positive cases of substance use disorder (sensitivity) and differentiate, or correctly fail to identify, non-disordered substance use (specificity) was assessed using a technique called area under the curve, which generates a single statistic ranging from 0-1 that captures how well a test performs. The closer a test is to 1, the more valid an indicator it is for that construct; substance use disorder diagnosis, in this case.
WHAT DID THIS STUDY FIND?
The module and clinicians were often aligned, especially with alcohol use disorder and tobacco use disorder
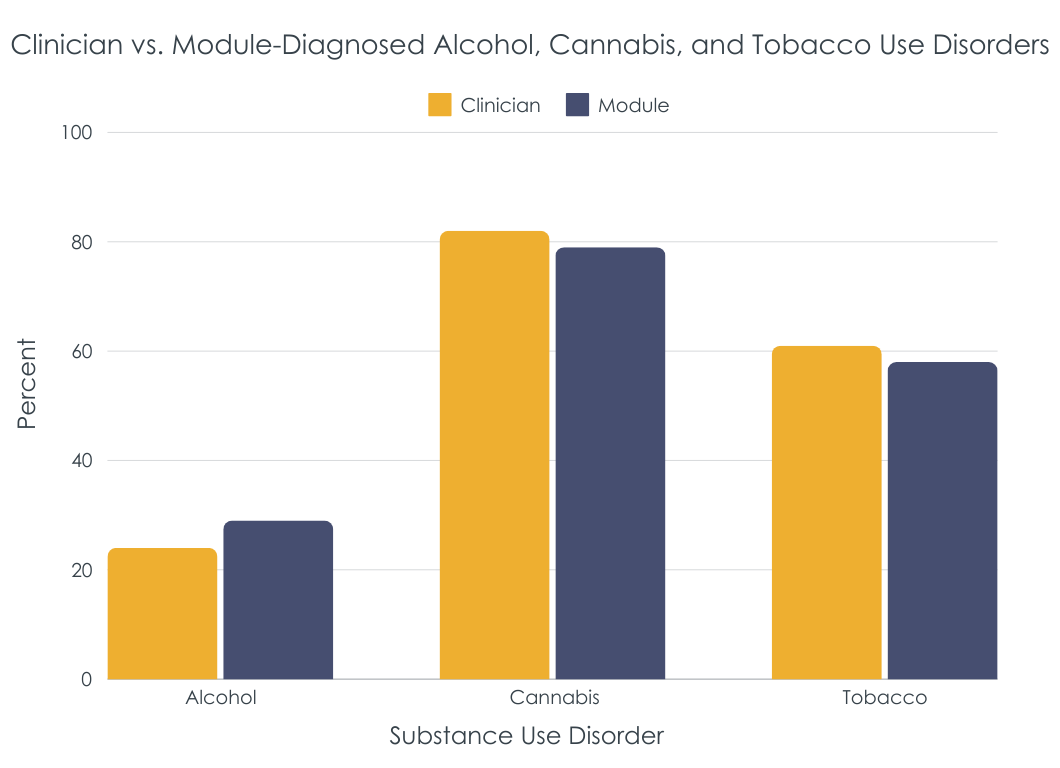
Among the 38 participants, clinicians diagnosed 9 (24%), 31 (82%), and 23 (61%) with alcohol use, cannabis use, and tobacco use disorders respectively. In contrast, the module identified 11 (29%), 30 (79%), and 22 (58%) with alcohol, cannabis, and tobacco use disorders. Proportions between the groups (clinician vs. module determined diagnosis) were not meaningfully different. However, the same individuals were not necessarily diagnosed by both the module and the clinician. There were 6 (16%), 26 (68%), and 18 (47%) that were identified with alcohol, cannabis, and tobacco use disorders by both clinicians and the module.
The module performed the worst with cannabis use disorder
The module was able to identify alcohol use and tobacco use disorders moderately well, with area under the curve values of about 0.75, suggesting the module correctly classifies adolescents about 75% of the time. Values between 0.7–0.8 are considered acceptable, while values of 0.8–0.9 are considered excellent. In contrast, the module was not able to discriminate cannabis use disorder as well based on an area under the curve value of 0.6. Values between 0.5–0.6 are considered nondiscriminatory.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study, adolescents completed the World Mental Health Composite International Diagnostic Interview Substance Abuse Module, a commonly used measure to identify individuals with a substance use disorder, and were also evaluated by a clinician for alcohol, cannabis, and tobacco use disorders. While overall numbers of cases diagnosed by clinicians versus a module were similar (see figure above), the rate of agreement for a given individual depended on the type of substance use being assessed. The module performed moderately well for alcohol and tobacco use disorders but poorly for cannabis use disorder. This means that the module may not appropriately identify adolescents with and without cannabis use disorder. Adolescents are at a unique stage of development, and substance use disorders may present differently. Adolescents may also perceive the diagnostic criteria differently. For example, they may not recognize patterns of their behavior or appropriately attribute consequences to their substance use.
Cannabis use and the disorder criteria may be particularly nuanced for adolescents due to their developmental stage. Appropriately understanding substance use disorder criteria, especially cannabis use disorder, for adolescents likely requires additional research.
Previous studies highlighted how cannabis use among youth can be harmful and yet is increasing nationally. For example, cannabis use among youth is linked to worse learning, attention, and executive functioning. Cannabis use disorder is also uniquely associated with suicidal behaviors among youth. Recreational cannabis legalization for adults has also been found to increase the likelihood of youth cannabis use. The results from this study suggest that a commonly used measure functions poorly in identifying those with and without cannabis use disorder. Further evaluation is needed to understand the nuance of cannabis use disorder among adolescents and how to screen for it.
Individuals’ first experiences with substance use often occur during adolescence. Use can escalate from experimentation to use associated with a range of immediate and prolonged consequences (e.g., worse academic grades, delayed workforce entry). Identifying adolescents with a substance use disorder early is important to connect those individuals with the appropriate services (intensive outpatients, residential treatment, etc.) as well as craft public health responses to substance use. Many adolescents also use multiple substances, so distinguishing between alcohol, cannabis, and tobacco use disorders can further help target treatment. The findings from this study further highlight the need to expand research into developmentally appropriate screening and diagnostic tools.